
ARGUMENTS AGAINST THE RULE OF FEAR
My german bestseller finally in English!
Get your copy of 'False Pandemics: Arguments Against the Rule of Fear'. Available in both eBook and paperback.
Discover the truth behind the pandemic power grab and arm yourself with the knowledge to challenge false health narratives.
Grab your digital copy on Amazon now, available for immediate download!"
Prefer a tangiable copy? Secure your copy of the paperback edition at OVAL.media Shop .
(Please note: High shipping costs may apply outside of Europe.
Source: Doctors for COVID Ethics
Why intramuscular COVID-19 vaccination must fail
Anonymous, MD,* Sucharit Bhakdi, MD, and Michael Palmer, MD
December 7, 2021,†
Abstract
Many countries are currently experiencing a wave of COVID-19 “breakthrough cases” in spite
of high vaccination rates. In this paper, we explain the fundamental reason why such cases
had to be expected: the antibodies induced by intramuscular vaccination will only circulate in
the bloodstream, but they will not reach the surface of the mucous membranes in the upper
airways. We also briefly discuss possible mechanisms of vaccine-induced immunopathology.
1 Introduction: All antibodies are not created equal
There are different types of antibodies utilized by the human immune system. The major
ones are IgM, IgG and IgA [1]; there are two other classes, IgD and IgE, but there is no need to
discuss them here.
IgM is generated in the early stages of an adaptive immune response and is then gradually
replaced with IgG antibodies. Both IgM and IgG circulate mainly in the bloodstream. IgG is
the most abundant antibody in the blood. On the other hand, while some IgA is found in the
bloodstream as well, most IgA is secreted across the mucous membranes of the respiratory
tract and the gut, which it then covers and protects.
When our immune system is confronted with an invading pathogenic microbe, the predominant
type of antibody it produces depends on the location of that pathogen. If the pathogen
is encountered in the bloodstream or inside of tissues within the body, e.g. the muscle, then
the immune system will produce mainly IgG antibodies, which will accumulate in the bloodstream.
On the other hand, if the pathogen is introduced through the respiratory tract (e.g.
the nostrils), then the immune system will produce mainly IgA antibodies—to be more specific,
secretory IgA, or sIgA.
While sIgA dominates in the upper airways, some IgG is found along with IgA in the lower
airways, that is, the bronchi and lung alveoli. In addition to sIgA, an immune response triggered
by a respiratory tract infection will also generate both IgG and IgA within the bloodstream,
which provides a safeguard in case the barriers of the respiratory tract are breached
and the pathogens enter the tissues. In short, sIgA is the main antibody the immune system
relies on in the upper respiratory tract (URT), and it forms the first line of defense against
respiratory pathogens.
2 Why is sIgA antibody important?
The key reason why an sIgA-based antibody response is desired against respiratory pathogens
is that sIgA does not promote inflammation. Binding of sIgA antibodies to the antigens (such
as viruses or bacteria) leads to “quiet” expulsion of these pathogens from the body, but it does
not elicit any additional damaging immune responses. In contrast, an IgG-based response is
followed by an inflammatory immune reaction. This reaction is triggered by a change in the
molecular shape of the Fc region (the tail end) of IgG antibodies, which causes them to activate
inflammatory cells as well as the serum complement system.
Since our respiratory tract constantly encounters viruses and bacteria within the air we
inhale, IgA-based immune responses help avoid unnecessary and repeated inflammations in
our airways. sIgA in the mucous membranes of the respiratory tract can subdue the infection
and stop the transmission of these germs safely.
Considering these well-established scientific facts, it is beyond perplexing that people only
talk about antibodies (mainly IgG antibodies) in the bloodstream after COVID vaccination. If
a vaccine should protect us from respiratory viruses and from transmitting them to others, it
should elicit an IgA-based immunity in our respiratory tract, especially in the upper airways.
3 What is really damaging our body: viruses, or our own immune system?
Respiratory viruses rarely cause direct damage to our body. It is typically the overreaction
of our immune system against those viruses that does the damage [2, 3]. With respect to
COVID-19, a recent paper on the causation of clinically severe disease sums it up as follows
[4]: [Severity of COVID-19] is suggested not to be a direct effect of viral infection but instead to be
caused by the over-activation of the immune system in response to infection, because worsening
of disease coincides with the activation of adaptive immunity. This excessive immune response
is frequently described as a “cytokine storm” . . . Together, high pro-inflammatory cytokines,
known to induce collateral damage to tissues, and muted anti-viral responses suggest that an
unfavorable immune response may be driving disease in patients with severe cases of COVID-19.
4 The route of vaccination matters
A vaccine that is given by intramuscular (IM) injection will mainly induce IgG antibodies in
the blood; this matches the body’s response to pathogens introduced by the same route. It
is well known that IM vaccines generate very little or no sIgA in the respiratory tract. Therefore,
IM injection is not an efficient way of prepping our immune system against respiratory
viruses. Should a full-blown pneumonia develop, circulating IgG antibodies will seep out of
the capillaries into the alveoli and there help with viral clearance; therefore, conceivably an IM
injection might afford some measure of protection against severe disease. On the other hand,
vaccine-induced IgG antibodies may also cause exacerbate the disease (see next section). In
any case, prior to inflammation, practically no IgG will be present on the respiratory mucous
membranes, which leaves them vulnerable to infection. This is why the current COVID-19 vaccines
cannot prevent infection or transmission of the virus [5, 6]. Below is a direct quote from
the review paper by McGhee et al. [6]:
It is surprising that despite our current level of understanding of the common mucosal immune
system, almost all current vaccines are given to humans by the parenteral route. Systemic immunization
is essentially ineffective for induction of mucosal immune responses. Since the majority
of infectious microorganisms are encountered through mucosal surface areas, it is logical to
consider the induction of protective antibodies and T cell responses in mucosal tissues.
Note that this statement was made already three decades ago—yet nothing has changed,
and the same flawed, outdated approach of intramuscular injection has been adopted yet again
with the “modern” and “high-tech” COVID-19 vaccines.
We can conclude that either the natural infection through our respiratory tract or nasal
vaccination is required to induce effective immunity against respiratory viruses. With COVID-
19, this is borne out by a recent animal study [7], which confirmed that the AstraZeneca COVID
vaccine administered by the intramuscular route failed to protect hamsters from the infection
by SARS-COV-2 or to prevent the transmission of this virus. When the vaccinated animals were
challenged with the virus through the airways, they still became infected, and their lungs were
damaged. On the other hand, the animals that were vaccinated by the nasal route were able to
clear the viruses in the URT and prevent the infection in the lower respiratory tract (LRT).
The lack of protection against infection of the airways by serum IgG is not limited to
SARS-CoV-2 and COVID. As early as 1984, Liew et al. demonstrated that the IgG found in the
bloodstream is quite irrelevant for the protection against influenza virus; it is the sIgA on the
mucous membranes that prevents the virus from establishing infection.
In conclusion, sIgA on the mucous membranes, especially in the URT, is necessary for
effective and protective immunity against respiratory viruses, and it is induced only when the
antigen is introduced via the natural route—into the URT itself. This rule applies to both
natural pathogens and vaccines.
5 An IgG response can be a bad thing
Not only does IgG circulating in the bloodstream fail to prevent infection with respiratory
viruses, but an IgG-based immune response can even elicit harmful inflammatory responses,
causing serious tissue damage within the respiratory tract. In their recent review article on
mucosal immunity to COVID-19, Russell et al. state [8]:
Most attention has been given to virus-neutralizing antibodies, especially circulating antibodies.
However, these can only be effective in the prevention of infection or disease if [the antibodies]
reach the mucosal surfaces where the virus is present, and it should be noted that circulating
IgA, even in polymeric form, is not effectively transported into secretions. While plasma-derived
IgG occurs in the URT and especially the lower respiratory tract (LRT), IgG is inflammatory in its
mode of action, by the induction of such effector mechanisms as complement activation and the
engagement of phagocytes such as macrophages and neutrophils as well as natural killer (NK)
cells. The serious pathology of COVID-19 occurs in the terminal airways of the lungs, where circulating
IgG is the dominant immunoglobulin. The resulting intense inflammation involves multiple
molecular and cellular factors, including cells recruited by virus-induced chemo-attractants.
In practical terms this means that intranasal immunization should be an effective means
of generating predominantly sIgA antibody responses in the URT and LRT, where SARS-CoV-2
could be neutralized and eliminated without inflammatory consequences. In addition, it implies
that assaying IgA antibodies in nasal secretions or saliva should be a more informative way
of assessing effective immune responses against SARS-CoV-2, whether induced by the natural
infection or by intranasal immunization. Assaying serum IgA antibodies, while of additional
interest, is not a substitute, because serum IgA comes from a different source (mainly the bone
marrow) and consists mostly of monomeric IgA1. This is distinct from mucosal sIgA, which . . .
is locally synthesized by pIgA-secreting plasma cells resident in the subepithelial spaces (lamina
propria) of mucosal tissues and glands . . . Moreover, sIgA is essentially non-inflammatory, even
anti-inflammatory, in its mode of action. IgA does not activate complement . . .
An association of excessive IgG-based immune responses with negative clinical outcomes
has also been observed after natural infection with SARS [9] and COVID-19 [4, 10]. IgG antibodies
will bind to virus particles first and then, via their Fc moieties (see Section 2), to Fc
receptors on immune cells. The virus may then enter those cells and subsequently replicate
within them. This disease mechanism is known as antibody-dependent enhancement and also
occurs with other virus families [11].
In addition to aggravating acute lung disease such as in SARS and COVID-19, high concentrations
of IgG are also associated with chronic inflammatory lung diseases such as idiopathic
pulmonary fibrosis and chronic hypertensive pneumonitis [12]. In summary, too little IgG is a
bad thing, but too much IgG is equally a bad thing.
6 Vaccination and M1/M2 macrophages
Macrophages are an important type of innate immune cells; their role is to ingest and destroy
pathogenic microbes. Macrophages can adopt either an M1 or M2 type, depending on
the inflammatory state of the tissue. M1 macrophages promote inflammation, whereas M2
macrophages promote wound-healing. Thus, the balance between M1 and M2 macrophages is
essential for a healthy immune system.
A recent study in monkeys has demonstrated that the intramuscular injection of a vaccine
against SARS-COV—the original SARS virus from 2003, which is highly homologous to the
causative agent of COVID (SARS-CoV-2)—promoted the elimination of virus particles that were
injected directly into the trachea, but also caused severe inflammatory injuries in the lung
tissues. Inflammation was exacerbated by a shift of macrophage polarization from woundhealing
M2 toward inflammatory M1 macrophages [13]. Priming the lung macrophages into
M1 type leads to dangerous inflammatory diseases and tissue damages, and that’s what the
IM vaccination does according to this paper.
7 Vaccination and Th2-type immunopathology
T helper cells are a type of lymphocytes that plays a key role in the stimulation and regulation
of immune responses. Again, there are two major subsets of this cell type, referred to as Th1
and Th2, respectively. Th1 cells activate immune responses against intracellular pathogens,
including protozoa, bacteria, and viruses. Th2 cells, on the other hand, help mount a defense
against infections with worm parasites, but they also promote allergic diseases such as asthma,
atopic dermatitis, and hay fever [14]. A hallmark of Th2-activated responses is an increased
abundance in blood and tissues of eosinophil granulocytes. These effector cells are useful for
combating worm parasites, but for little else; in allergic disease, they merely contribute to the
tissue damage.
It is therefore significant that several experimental vaccines against the original SARS virus,
while inhibiting proliferation of the virus within the lungs to some degree, caused Th2-type
lung pathology, characterized by increased numbers of eosinophil granulocytes within and
aggravated injury to the lungs [15–17]. These results indicate that the experimental vaccines
against SARS-CoV may cause more severe illnesses when the vaccinated person is challenged
with the real virus.
We must stress again that SARS-CoV and SARS-CoV-2 are highly homologous, which means
that any risk or problem known with SARS-CoV must be considered with SARS-CoV-2 also.
While the manufacturers Pfizer, Moderna, and Johnson&Johnson claim that their vaccines
preferentially induce Th1 responses, supporting data from human vaccinees are scarce or
lacking altogether [18–20].
8 Conclusion
All of the currently used COVID vaccines are applied by intramuscular injection, and they
are therefore unable to prevent infection of the upper airways with the SARS-CoV-2 virus. In
fact, in their clinical trials, none of the manufacturers even attempted to demonstrate efficacy
against infection or transmission in their clinical trials [18–21], and the total lack of efficacy
in the real world has since been documented in a large study published by the CDC [22].
The vaccines can, however, lead to severe respiratory immune disease, including Th2-type
immunopathology and autoimmunity. When factoring in the large number of adverse events
that are being reported with the current vaccines and the low case fatality rate of COVID-19,
which we have discussed elsewhere [23], it is clearly more scientific and more reasonable to
strive for herd immunity by natural infection rather than vaccination.
*The first draft of this document was written by a colleague who prefers to remain anonymous.
†In this updated version, a misleading statement in Section 4, pertaining to the location of IgG in the airways, has been
amended.
References
[1] Anonymous: Antibody. 2021. url: https://en.wikipedia.org/wiki/Antibody.
[2] A. H. Newton et al.: The host immune response in respiratory virus infection: balancing virus
clearance and immunopathology. Semin. Immunopathol. 38 (2016), 471–482. doi: 10 . 1007 /
s00281-016-0558-0.
[3] M. Z. Tay et al.: The trinity of COVID-19: immunity, inflammation and intervention. Nat. Rev.
Immunol. 20 (2020), 363–374. doi: 10.1038/s41577-020-0311-8.
[4] W. Hoepel et al.: High titers and low fucosylation of early human anti-SARS-CoV-2 IgG promote
inflammation by alveolar macrophages. Science translational medicine 13 (2021). doi: 10.1126/
scitranslmed.abf8654.
[5] Y. Kurono: The mucosal immune system of the upper respiratory tract and recent progress in
mucosal vaccines. Auris, nasus, larynx (2021). doi: 10.1016/j.anl.2021.07.003.
[6] J. R. McGhee et al.: The mucosal immune system: from fundamental concepts to vaccine development.
Vaccine 10 (1992), 75–88. doi: 10.1016/0264-410x(92)90021-b.
[7] N. van Doremalen et al.: Intranasal ChAdOx1 nCoV-19/AZD1222 vaccination reduces viral shedding
after SARS-CoV-2 D614G challenge in preclinical models. Science translational medicine 13
(2021). doi: 10.1126/scitranslmed.abh0755.
[8] M. W. Russell et al.: Mucosal Immunity in COVID-19: A Neglected but Critical Aspect of SARSCoV-
2 Infection. Front. Immunol. 11 (2020). doi: 10.3389/fimmu.2020.611337.
[9] N. Lee et al.: Anti-SARS-CoV IgG response in relation to disease severity of severe acute respiratory
syndrome. J Clin Virol 35 (2006), 179–184. doi: 10.1016/j.jcv.2005.07.005.
[10] W. Tan et al.: Viral Kinetics and Antibody Responses in Patients with COVID-19. medRxiv (2020).
doi: 10.1101/2020.03.24.20042382.
[11] H. Ulrich et al.: Dengue Fever, COVID-19 (SARS-CoV-2), and Antibody-Dependent Enhancement
(ADE): A Perspective. Cytometry A 97 (2020), 662–667. pmid: 32506725.
[12] H. Y. Reynolds et al.: Analysis of cellular and protein content of broncho-alveolar lavage fluid
from patients with idiopathic pulmonary fibrosis and chronic hypersensitivity pneumonitis. J.
Clin. Invest. 59 (1977), 165–175. doi: 10.1172/jci108615.
[13] L. Liu et al.: Anti-spike IgG causes severe acute lung injury by skewing macrophage responses
during acute SARS-CoV infection. JCI insight 4 (2019). pmid: 30830861.
[14] M. J. Butcher and J. Zhu: Recent advances in understanding the Th1/Th2 effector choice. Faculty
reviews 10 (2021), 30. pmid: 33817699.
[15] M. Bolles et al.: A double-inactivated severe acute respiratory syndrome coronavirus vaccine provides
incomplete protection in mice and induces increased eosinophilic proinflammatory pulmonary
response upon challenge. J. Virol. 85 (2011), 12201–15. pmid: 21937658.
[16] C.-T. Tseng et al.: Immunization with SARS coronavirus vaccines leads to pulmonary immunopathology
on challenge with the SARS virus. PLoS One 7 (2012), e35421. pmid: 22536382.
[17] N. Iwata-Yoshikawa et al.: Effects of Toll-like receptor stimulation on eosinophilic infiltration in
lungs of BALB/c mice immunized with UV-inactivated severe acute respiratory syndrome-related
coronavirus vaccine. J. Virol. 88 (2014), 8597–614. pmid: 24850731.
[18] Anonymous: EMA Assessment report: COVID-19 Vaccine Janssen. 2021. url: https : / / www .
ema.europa.eu/en/documents/assessment-report/covid-19-vaccine-janssen-eparpublic-
assessment-report_en.pdf.
[19] Anonymous: EMA Assessment report: COVID-19 Vaccine Moderna. 2021. url: https://www.
ema.europa.eu/en/documents/assessment-report/spikevax-previously-covid-19-
vaccine-moderna-epar-public-assessment-report_en.pdf.
[20] Anonymous: EMA Assessment report: Comirnaty. 2021. url: https://www.ema.europa.eu/en/
documents/assessment-report/comirnaty-epar-public-assessment-report_en.pdf.
[21] Anonymous: EMA assessment report: COVID-19 Vaccine AstraZeneca. 2021. url: https://www.
ema.europa.eu/en/documents/assessment-report/vaxzevria-previously-covid-19-
vaccine-astrazeneca-epar-public-assessment-report_en.pdf.
[22] C. M. Brown et al.: Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough
Infections, Associated with Large Public Gatherings—Barnstable County, Massachusetts, July
2021. MMWR. Morbidity and mortality weekly report 70 (2021), 1059–1062. pmid: 34351882.
[23] M. Palmer and S. Bhakdi: Expert statement regarding the use of Moderna COVID-19-mRNA-Vaccine
in children. 2021. url: https://doctors4covidethics.org/expert-statement-regardingthe-
use-of-moderna-covid-19-mrna-vaccine-in-children/.
IMPORTANT DRUG INFORMATION
Berlin, 23.8.2021 (in the context of the base camp planning game)
Injections for immunisation against COVID-19
All genetically engineered drugs with mRNA or vector technology from the companies
(BioNtech/Pfizer, Moderna, AstraZeneca, Johnson&Johnson/Janzen-Cilag)
Description of the mode of action
All four drugs are based on procedures that target changes in cells of the human body. By introducing nucleic acid sequences by means of lipid nanoparticles (BioNtech/Pfizer, Moderna) or recombinant, i.e. genetically modified viruses, so-called vectors (AstraZeneca, Johnson&Johnson), the cells of the treated are stimulated to produce parts of SARS-CoV-2 viruses (spike proteins) and to present them to the passing blood, which are to be recognised and rejected by the immune system. This should result in antibody formation that protects against damage caused by infection with wild SARS-CoV-2 viruses.
BENEFIT ASSESSMENT
These procedures have been used in humans in practice for the first time since December 2020. The experience prior to the emergency use market approvals given by the regulatory authorities was limited to a few months in 2020.
Through comparisons with untreated control groups, the number of people to be treated per avoided case of infection was around 100 people (NNV approximately between 60 and 140). This corresponds to an absolute protective effect of around 1% [1].
Due to the small number of study participants and the short observation periods, however, these values of the applicant companies should be viewed with reservation. However, they seem to fit with the fact that the incidence of symptomatic cases previously observed in the population was also around 1% per season. This fits with a stable cross-immunity against coronaviruses found in several studies in more than 90% of the population [2].
A differential diagnostic differentiation of symptomatic cases from symptoms caused by other respiratory pathogens has hardly been done so far, or only in special cases. However, since corona infections always make up only a subset of influenza cases, the number of cases of corona infections cannot be greater than the total number of acute respiratory illnesses observed.
In addition to the known older corona variants, different beta corona viruses such as the SARS successors have been spreading worldwide for more than 15 years. For a few months at a time, individual new variants dominate, but still do not differ significantly in their pathogenicity epidemiologically [3].
The current injections - as can now be seen - hardly change anything about the possibility of becoming infected via the respiratory tract and transmitting the pathogens to others. Even in the case of possibly initially dangerous viruses, there is regularly a weakening of the pathogenicity, as this brings evolutionary advantages to the emerging variants. Resistance (as with bacteria to antibiotics) therefore plays no role in the risk assessment of viruses.
On epidemiological relevance
The numerous PCR screening tests for SARS-CoV-2 are not useful for determining and recording infections and contagiousness without further diagnostics. The numbers collected with them give a completely useless picture due to inevitably many false positive tests and non-standardised procedures in laboratory practice and are irrelevant in terms of infection epidemiology.
Summary benefit assessment:
A significant protective effect for public health cannot be expected from the four medicinal products mentioned.
RISK ASSESSMENT
In principle, injectable drugs for immunisation against respiratory pathogens are a risky and unpromising approach, since the defence against these viruses normally occurs first and predominantly successfully in the upper respiratory tract. In healthy individuals, sufficient local defence mechanisms of the innate and acquired immune system are located here. The intramuscular administration of antigens or even the genetic stimulation of antigen formation somewhere inside the body is an "attack through the back door" and involves considerable risks for a coordinated immune defence.
The antigens to be formed by the body itself are spike proteins, as they are also found on the envelope of coronaviruses. Spike proteins enter the blood extremely rarely during a respiratory infection with coronaviruses. But only then do they lead to "vascular disease. The spike proteins that are genetically produced in the body after the injection are also highly toxic and cause symptoms similar to those known from otherwise rare severe courses of corona.
The distribution of the injected nanoparticles or vectors in the body apparently changes from application to application and is also key to possible side effects. Sufficient studies on the targets, i.e. the cells and tissues that are genetically modified, are not available. In leaked animal studies from Japan, a worrying accumulation of nRNA-containing nanoparticles was also found in the ovaries, for example [4](5). This could lead to infertility. Other findings and side effects suggest that the heart muscle, the veins of the brain (sinus venosus) and the digestive organs (mesenteric veins), among others, are also targets of these drugs. Health professionals have therefore now been asked to be alert to signs and symptoms of thromboembolism and/or thrombocytopenia (shortness of breath, chest pain, leg swelling, leg pain or persistent abdominal pain, severe or persistent headache, blurred vision, confusion, seizures, petechiae). Treated persons should be adequately informed and seek medical attention immediately if such symptoms occur.
Immunological attacks on the vascular wall cells that have been altered by the injected RNA and then present spike proteins destroy them and trigger microthrombotic chain reactions that destroy the sections of tissue that are then less well supplied with blood. Particularly in the heart, brain, gonads and areas of the intestine, this can lead to irreversible failures with corresponding symptoms.
In the meantime, there are more and more systematic observations that show that up to half of those treated suffer from such intravascular microthromboses. Indications for this are provided by the determination of coagulation parameters (increase in D-dimers and decrease in platelet count), which is now also increasingly carried out by doctors before and after injections. A corresponding systematic monitoring of such risks has not yet been published by the competent authorities.
In animal experiments, the unnatural contact of the immune system with spike antigens has repeatedly led to an erroneous reaction with increased viral reproduction (ADE) and an unchecked defence reaction (cytokine storm) when exposed to wild viruses. Such an infection, promoted and intensified by incompletely neutralising antibodies, is life-threatening. Other ingredients of the drugs, such as nanoparticles or polyethylene glycol (PEG), can also lead to severe side effects, which will not be discussed here.
The number of adverse drug reactions (ADRs) has meanwhile reached alarming proportions and far exceeds any previously observed for vaccinations. As of 31 July 2021, over 20 000 deaths and approximately 2 million ADRs had been reported to the EMA alone. However, it is known that only a small proportion of ADRs are even recognised or reported. Experience shows that the number of unreported cases is many times higher. The number and severity of adverse drug reactions increase with each injection.
Summary risk assessment:
The side effects known so far and further expected harm to those treated clearly outweigh any recognisable benefit.
Conclusions:
1. the use of the above-mentioned medicinal products should be discontinued immediately.
2. the requirements for an emergency use marketing authorisation are not fulfilled.
3. existing stocks should be confiscated by the medicines inspectorate and subjected to a systematic, batch-by-batch content analysis.
4. the medical profession should be more widely informed about possible ADRs and motivated to participate in their timely detection and in the prevention of harm.
5. sufficient specialised centres should be made available for the counselling and treatment of those affected.
6. To protect against corona infections in the future: accurate diagnosis of symptomatic patients to indicate self-isolation at home for up to 14 days with all supportive treatments.
Notes and sources:
[1] The companies' reported protective effects (RRR) of over 60% to 95% is useless for benefit assessment. If, for example, one case of infection occurs in the control group of 20,000 untreated people and none in the prophylactically treated group, the relative risk reduction would be 100% even though 20,000 people had to be treated to prevent only one case. (The NNV would be 20000).
[2] An easy-to-understand summary of cross-immunity with numerous literature references can be found here: https://christianhannig.medium.com/auf-dem-weg-zum-verfassungsgericht-teil-1-von-n-formale-anforderungen-7c80f793c68b.
[3] This also applies to the temporarily dominant "delta" variant.
[4] https://freewestmedia.com/2021/06/04/pfizer-biontech-animal-trials-show-dangerous-concentrations-of-nano-particles-in-organs/
(5)Alana F Ogata, Chi-An Cheng, Michaël Desjardins, Yasmeen Senussi, Amy C Sherman, Megan Powell, Lewis Novack, Salena Von, Xiaofang Li, Lindsey R Baden, David R Walt, Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients, Clinical Infectious Diseases, 2021; , ciab465, https: //doi. org/10.1093/cid/ciab465
Dangerous side effects of genetically induced production
of SARS CoV-2 spike proteins
Wolfgang Wodarg 15.3.2021
Neither Coronaviruses nor their spikes do enter blood in uncomplicated infections. In more than 90% of all corona-infections immune barriers in the upper respiratory tract or local mucosa immunity will prevent this. This is the result of T-cell driven cross-immunity. (1)
We do not find such an immunity by analyzing antibodies, instead we would have to analyze many T- cell epitopes of corona viruses (2), which is an effort to big to be used for preventive public health reasons.
No matter, which new mutation of a virus will come, the cellular memory of the local immune system is able to recognize tens of different typical epitopes of each respiratory virus species, even then, when some of them have changed by mutations (2).
This seems to be true for all mild respiratory infections and not just for coronaviruses*.
In rare cases of insufficient local immunity, or by medical manipulations (intubation!) viruses happen to enter the blood and become targets of a stronger and more generalized immune defence with humoral and cellular traces (e.g. antibodies) and symptoms like fever or even hampered organ function (less than 1%) (3).
If coronaviruses reach blood, the effect of corona-Spikes within the blood system is well known to be the reason for complicated or deadly Corona infection courses. Some of them are seen as a direct effect in reaction with certain cell receptors, others are reported as secondary effects, happening when infected cells start reproducing new viruses.
All those reactions take place or start within some days or in the first weeks after the infection. Those effects may be the reason for the fact that even some younger patients are dying each year with atypical pneumonia, heart or central nervous complications after some infection with different flu viruses like Influenza A or B, Parainfluenza, human Metapneumovirus, RS-Virus, Coronavirus and many others.
It is well known that also virus-virus synergism as well as superinfections with bacteria or nosocomial infections may play an important role in those rare complications among children and younger adults. Very often there are other pathogenetic factors that lead to complications. All those cases have to be distinguished from elderly victims, where frailty und chronic diseases weaken the resistance against any additional infectious stress.
No matter, where those corona-spikes come from, whether they are part of whole viruses or just spike-proteins, produced by genetically programmed cells, in both cases dangerous reactions may result, if they reach the patient’s blood vessels.
Again, a normal acute respiratory infection without fever or severer symptoms (> 99%) does not come along with corona-spike protein reaching the blood and does not initiate risky generalized immune alarms.
However when genetically engineered vectors or particles are injected into the upper arm muscle, natural immune barriers or systems of defence are bypassed.
There are not enough competent immune cells in the tissue of the m. deltoideus. And as soon as some closer cells in the muscle start to produce and present spike protein, there should be a strong and more and more generalizing local immune reaction with swellings and pain. This fits well with observed side effects of the ongoing experimental use of all genetically modifying injections.
It is unknown where the new self-made spike proteins remain, or whether parts of them could go with the blood. As there are many blood vessels in the muscle, it may happen often and easily, that part of the injected dose reaches the blood already during injection.
If this happens, the complications may be similar to those, coming along with hematogenous sowing during a complicated infection.
In such cases there are three possible risks of vaccination, that can have similar serious consequences and even may happen in combination with each other:
1.
after intramuscular injection, it must be expected that at least in some cases the injected genetic information may leave the injection site by mistake or accidentally and more or less enter the bloodstream to be spread throughout the body [1].
In such cases, it must be also expected that the genetic information will be distributed in the bloodstream and taken up by endothelial cells in different parenchymatic organs. Endothelic cells are those cells, with which blood vessel walls are lined. It can be assumed, that such uptake in endothelial cells occurs particularly at sites with slow blood flow. This will presumedly happen, where the contact time is long enough, such as during capillary passage or in the venous system following with low pressure and orthostatic narrow venous network.
When this happens, the injected genetic information will cause those endothelial cells to produce portions of spike proteins and present them on their surfaces to passing blood cells.
Many healthy individuals have CD8 lymphocytes that patrol the blood and recognize such corona spike peptides, which may be due to previous COVID infection but also to cross-reactivity with other coronavirus types [6; 7] [8].
We must assume that these CD8 lymphocytes launch an attack on the corresponding cells upon contact. This can lead to vascular wall damage at countless sites in the body with subsequent triggering of blood clotting by activation of platelets (thrombocytes). This is what happens when the vaccine itself enters the blood.
2.
when such spike proteins, genetically engineered from our cells, enter the blood, they directly bind with the ACE2 receptors of platelets, which also leads to blood clotting and thrombosis [9][10]. This has also been observed with whole coronaviruses entering the blood in rare cases. Thrombocytopenia so developed has also been reported in vaccinated individuals [11][12][13].
3.
In addition: the ability of the SARS-CoV-2 spike proteins to initiate cell fusions is very strong. The resulting giant cells can also lead to vasoobstruction, inflammatory responses, and microthrombosis. (14)
Manifestations of all three risks
On blood tests, it can be seen by a drop in platelet count and the appearance of D-dimers (fibrin degradation products) in the blood. Clinically, there can be innumerable damages as a result of circulatory disorders throughout the body, including the brain, spinal cord and heart. Because of such consumption of clotting factors and platelets, hemorrhage can also occur in various organs and have fatal consequences, for example, in the brain.
Importantly, for all of the above possibilities that can lead to disseminated intravascular coagulation (DIC), all three vaccines lack evidence that those risks have been excluded by the EMA prior to their approval for use in humans.
*Patients admitted to hospitals with atypical viral infections usually also have multiple infections (12), but unfortunately, especially in times of fixation on Covid-19, these are rarely clarified by differential diagnosis.
**The first two questions presented have also been submitted to the European Medicines Agency by an international group of scientists on 2/28/2020.
References:
(1) Zhou et al. BMC Infectious Diseases 2013, 13:433, http://www.biomedcentral.com/1471-2334/13/433
(2) SARS-CoV-2-derived peptides define heterologous and COVID-19-induced T cell recognition, Nature immunology.
(3) Systemic and mucosal antibody responses specific to SARS-CoV-2 during mild versus severe COVID-19 Cervia, Carlo et al. Journal of Allergy and Clinical Immunology, Volume 147, Issue 2, 545 - 557.e9
(4) Hassett, K. J.; Benenato, K. E.; et al.(2019).Optimization of Lipid Nanoparticles for Intramuscular Administration of mRNA Vaccines, Molecular therapy. Nucleic acids 15 : 1-11.
(5) Chen, Y. Y.; Syed, A. M.; MacMillan, P.; Rocheleau, J. V. and Chan, W. C. W.(2020). Flow rate affects nanoparticle uptake into endothelial cells, Advanced materials 32 : 1906274.
(6) Grifoni, A. et al.(2020). Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals, Cell 181 : 1489-1501.e15.
(7) Nelde, A.; Bilich et al (2020). SARS-CoV-2-derived peptides define heterologous and COVID-19-induced T cell recognition, Nature immunology.
(8) Sekine, T. et al.(2020). Robust T Cell Immunity in Convalescent Individuals with Asymptomatic or Mild COVID-19, Cell 183 : 158-168.e14.
(9) Zhang, S.; Liu, Y.; Wang, et al.(2020). SARS-CoV-2 binds platelet ACE2 to promote thrombosis in COVID-19, Journal of hematology & oncology 13 : 120.
(10) Lippi, G. et al. 2019 (COVID-19) infections: a meta-analysis, Clin. Chim. Acta 506 : 145-148.
(11) Grady, D. (2021). A Few Covid Vaccine Recipients Developed a Rare Blood Disorder, The New York Times, Feb. 8, 2021.
(12) Geoffrey D. Wool,: The Impact of COVID-19 Disease on Platelets and Coagulation, DOI: 10.1159/000512007.
(13) Giannis D, Ziogas IA, Gianni P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J Clin Virol. 2020 Jun; 127: 104362.
(14) Theuerkauf et al, iScience 24, 102170, March 19, 2021[12]Nickbakhsh, Sema, (2019 ) Virus-virus interactions impact the population dynamics of influenza and the common cold, www.pnas.org/cgi/doi/10.1073/pnas.1911083116
(15) Virus-virus interactions impact the population dynamics of influenza and the common cold, Sema Nickbakhsh, et al. (2019)MRC-University of Glasgow, Centre for Virus Research
My Letter to the Austrian Agency for Security in the Healthssystem 7.3.2021
Dear Sir or Madam,
contrary to your report, a strong tendency to thrombosis/microthrombosis is known as a side effect of spike proteins. And spike proteins are supposed to be produced in the body of all patients, genetically modified by Covid-19 “vaccines”
Spike proteins coming with the whole virus are normally rendered harmless by the local immune response in the upper respiratory tract during a corona infection.
However, in "vaccination" this protective barrier is bypassed.
Moreover, in intramuscular vaccination, the target cells of the mRNA or vectors are not containable. Even with only local (m.deltoideus) expression of the spike proteins, their wide spread is also not sufficiently clarified.
If now because of " expected severe side effects " with thromboses (see below) a drug is to be brought hastily on the market, you will probably take these connections into account in your decisions. I would like to know why you seem to have considered this knowledge irrelevant in your statement.
The PEI has just published further pathomechanisms that could explain such deaths. (Theuerkauf et al.)
A copy of this letter will also be sent to the colleagues of the Paul Ehrlich Institute.
Please acknowledge receipt of my message.
With kind regards,
Dr. Wolfgang Wodarg
Ltd. medical director (retired)
Internist-Pneumologist, Social Medicine
Physician for hygiene and environmental medicine
Member of the German Bundestag from 1994 to 2009
Honorary Member of the Parliamentary Assembly of the Council of Europe
Here is my publication on the subject:
Study with a drug against "expected" severe damage
6.3.2021 ww
On 1/29/2021 Mahmoud Ramadan mohamed Elkazzaz, from Kafrelsheikh University near Cairo submitted a study with isotretinoin to the NIH study registry under the number NTC04730895. This drug is intended to protect all vaccinated individuals whose cells produce corona spikes after gene vaccination from the expected severe side effects. This could be a big hit, because there are already about 5 million vaccinated people in Germany who could experience the announced severe side effects.
The application for the study[i] states:
Isotretinoin (13- cis-retinoic acid) versus spike protein-based vaccines for providing complete protection against COVID-19 and preventing the expected serious long-term side effects of the spike protein-based vaccine.
In a short time, the spike protein-based vaccine was approved as an emergency solution and is now being introduced. The spike protein-based vaccine provides guidance and signals for our cells to express a component of the so-called "viral spike protein." The strong interaction between angiotensin-converting enzyme 2 (ACE2) and the receptor binding domain (RBD) of the spike protein (SP) produced by the COVID-19 vaccine ,or found on the spike protein of viral particles, has an affinity (~10 nM), and this binding affinity is equivalent to that of many monoclonal antibodies (MAbs).
Therefore, the association of angiotensin-converting enzyme 2 (ACE2) with the binding domain of the spike protein is likely to be a strong and long-lasting interaction, and angiotensin-converting enzyme 2 (ACE2) is expected to enter antigen-presenting cells associated with the spike protein of COVID-19 vaccine or the spike protein of viral particles. (Translation and emphasis: WW)
The risk that the substance being tested seeks to reduce has been known for several months. In a large Chinese study published in the Journal of Hematology & Oncology as early as 9/4/2020[ii], well before the Covid-19 vaccines were approved or even used, it had been shown that the spikes of coronaviruses, when they enter the bloodstream, can do a great deal of damage, for example, by causing minute thromboses in the capillaries of many organs. Especially in the lungs such microthromboses are to be feared.
The Chinese study and also a study of the Paul-Ehrlich-Institute [iii]were carried out to show the world how dangerous coronaviruses are.
Coronaviruses and their spikes themselves are dangerous, but only if they get into the blood!
Fortunately, this is extremely rare unless the normally effective protective mechanisms in the upper respiratory tract have been bypassed or damaged by treatment or other circumstances.
High-risk side effects of genetic "vaccination" are concealed!
The vaccination, however, bypasses the natural barriers against coronaviruses and goes directly into the well supplied shoulder muscle. It is not known for sure whether the dangerous spike proteins are formed only there or whether other target cells are also stimulated to do so.
Such severe side effects of the current Corona vaccinations are not mentioned anywhere. Even the Paul Ehrlich Institute did not even mention them in its paper on the further risks of spike proteins (cell fusions) (see below).
In addition, there are possible dangerous immunological misreactions due to non-neutralizing antibodies with life-threatening effects, and furthermore the risk of becoming a victim of ADE (Antibody Dependent Enhancement) in case of a later contact with coronaviruses.
Meanwhile, reports of high excess mortality among the vaccinated are accumulating from Israel, Great Britain and Germany. A connection is criminally rarely thoroughly investigated but consistently brushed aside as non-existent.
In view of the minimal additional protection provided by vaccination, I consider the continuation of vaccination campaigns to be irresponsible and demand that they be stopped immediately.
[i] https://clinicaltrials.gov/ct2/show/NCT04730895
[ii] Zhang et al. Journal of Hematology & Oncology (2020) 13:120, https://doi.org/10.1186/s13045-020-00954-7
[iii] Theuerkauf et al, iScience 24, 102170, March 19, 2021 ª 2021 The Author(s). https://doi.org/10.1016/ j.isci.2021.102170
Incidents after
vaccination with AstraZeneca's COVID-19 vaccine
BAGS 07.03.2021
"The Federal Office for Safety in Health Care (BASG) has received two reports in temporal connection with a vaccination from the same batch (ABV 5300) of the AstraZeneca vaccine in the LK Zwettl:
a woman (49 y) has died as a result of severe coagulation disorders, another woman (35 y) who developed a pulmonary embolism is on the road to recovery.
Currently, there is no evidence of a causal relationship with vaccination. Based on the known clinical data, a causal relationship cannot be established because thrombotic events in particular
are not among the known or typical side effects of the vaccine in question. In the clinical data, even according to current knowledge, there are no data or signals of concern in this regard
compared to placebo...."
Was a dangerous side effect of vaccination ignored by the Paul Ehrlich Institute?
On 19 February, Angela Merkel announced at the G7 summit: "The pandemic is not over until everyone in the world has been vaccinated." The German government's top vaccination watchdog, Dr Klaus Cichutek, president of the Paul Ehrlich Institute (PEI), had published an article with a group of his staff just a few days earlier, that could significantly disrupt the chancellor's plans. The PEI researchers warn that in corona infections, the spines (spikes) of the coronaviruses can be responsible for major cell fusions with dangerous complications in various organs. This study was conducted at the same time as the testing of those vaccines that are supposed to induce the production of exactly such dangerous spikes - only without virus - in the cells of the "vaccinated". This does not sound good. But the warning paper does not even mention the vaccination with its spikes with a single word. Does the right hand not know what the left hand is doing at PEI?
WOLFGANG WODARG, 21 February 2021
The PEI research team, which also includes the director of this institute, Klaus Cichutek, had already submitted the article to the scientific journal iScience on 21 October 2020. On 5 February, the journal accepted it for publication. It is entitled: "Quantitative Assays Reveal Cell Fusion at Minimal Levels of SARS-CoV-2 Spike Protein and Fusion-from-Without, (FFWO)". A translated extract from the article can be read in the attached footnote (1).
This scientific paper, written with the participation of agencies director, is quite something, because it was apparently published in order to once again point out the special dangers of corona infections. These consist in the fact that the spike proteins of the coronaviruses alone can also fuse neighbouring cells, which can eventually form a clump of up to a hundred fused cells and perish in the process.
The work also found that the mere presence of the isolated spike proteins, without the viral body, can lead to such cell fusions on a large scale. (2) Such reactions have been known for some time, for example since the 1960s from the Newcastle disease virus (3), or subsequently from HIV viruses, where even parts of the envelopes are sufficient to cause such pathological cell fusions (4). The measles virus is also held responsible for such virus-induced cell clumps in the brain, and herpes viruses stimulate cell fusions that contribute to the typical skin changes.
The genetic "vaccines" currently in use shall programme the recipient's cells to produce just such spike proteins throughout the body. In which organs this happens cannot be predicted. It must therefore be feared that the strong tendency to uncontrollable cell fusions triggered by spike proteins can cause severe tissue damage and corresponding immunological and haematological consequences. Tissue destruction, microthromboses and secondary immune complications could result in severe clinical pictures and death within a short time.
It is completely
incomprehensible that the authors of the Paul-Ehrlich-Institute, who have precisely investigated and described the dangers of spike proteins, have not thought about what is caused by genetic
vaccinations. The PEI is also responsible for the safety of exactly those genetically engineered vaccines that are supposed to produce such spike proteins in the bodies of the
"vaccinated".
However, such an
obvious risk of vaccination is not even mentioned in the paper.
Clinical studies that explicitly observe or exclude such a risk with the vaccines are also not known. Of the adverse side effects known so far, several could well be explained by the fusion-from-without effect (FFWO). Further investigation seems urgently warranted. Vaccinated persons with side effects should be given the right to be examined immediately by an independent (!) body. If such a risk has not been ruled out, this would be another urgent reason to immediately stop all genetic "vaccinations" which are supposed to lead to the intracellular production and expression of spike proteins.
The PEI team further reports that, at least in the laboratory, the dangerous cell fusions could be significantly reduced by the administration of monoclonal anti-spike antibodies. Incidentally, Bill Gates mentioned the large-scale genetic production of such monoclonal antibodies for mass treatment in December last year.
Surely no one can want that: to make the complications with vaccinations, which would then have to be treated again with expensive monoclonal antibodies?
I would like to take this opportunity to point out the miserable risk-benefit profile of the "vaccinations" against Covid-19. For three genetic "vaccines" are currently being forced on many people by their governments after a hasty approval in a worldwide large-scale trial. All three are supposed to use slightly different technical processes to ensure, that after the injection our genetically modified cells produce such spikes as a vaccine themselves. This is cheaper and faster, so it brings more profits for the producers. But it is the first time that these technologies have been applied to humans.
Apparently, the Corona vaccinations do not have a great benefit. In the 19,000 vaccinated in the already poor BioNTech study, there were only 154 infections less than in the unvaccinated 19,000. The absolute risk of an infection was thus only reduced by less than 1 percent. In the vast majority of the population, there is cellular cross-immunity against anything that looks like Corona, even without vaccination. And even if a Corona infection were prevented by the vaccine, the other viruses would profit. They would then just have more space. All in all, it has also become clear in critical reviews that vaccinations against constantly changing seasonal respiratory viruses bring hardly any benefits, but risks. So now there is another one.
About the author:
Wolfgang Wodarg, MD, born in 1947, is a specialist for internal medicine and pulmonology, a specialist in hygiene and environmental medicine as well as in public health and social medicine. After his clinical work as an internist, he was, among other things, a director of a public health office in Schleswig-Holstein for 13 years, at the same time a lecturer at universities and technical colleges and chairman of the expert committee for environmental health at the Schleswig-Holstein Medical Association; in 1991 he received a scholarship to Johns Hopkins University, Baltimore, USA (epidemiology).
As a member of the German Bundestag from 1994 to 2009, he was initiator and spokesman in the Enquête Commission "Ethics and Law of Modern Medicine", member of the Parliamentary Assembly of the Council of Europe, where he was chairman of the Subcommittee on Health and vice-chairman of the Committee on Culture, Education and Science. In 2009, he initiated the committee of enquiry in Strasbourg on the role of the WHO in H1N1 (swine flu) and continued to be involved there as a scientific expert after leaving parliament. Since 2011, he has been working as a freelance university lecturer, doctor and health scientist and was voluntarily involved as a board member and health working group leader at Transparency International Germany until 2020. Further information can be found on his website.
Notes
(1) Here is the German translation of an excerpt of the article available as a preprint since 5 February 2021:
"Cell entry of the pandemic virus SARS-CoV-2 is mediated by its spike protein S. The most important antigenic determinant of cell entry is the spike protein S. The spike protein S is the antigen of the pandemic virus SARS-CoV-2. As the most important antigenic determinant, the S protein is the focus of various therapeutic strategies. In addition to particle-cell fusion, S mediates fusion between infected and uninfected cells, leading to the formation of syncytia. Here we present sensitive assay systems with high dynamic range and high signal-to-noise ratio, covering not only particle-cell and cell-cell fusion, but also "fusion from without" (FFWO). In FFWO, S-containing virus particles induce syncytia independently of de novo synthesis of S. Neutralising antibodies as well as sera from convalescent patients inhibited particle-cell fusion with high efficiency. In contrast, cell-cell fusion was only moderately inhibited, although S protein concentrations below the detection limit of flow cytometry and Western blot were required. The data suggest that syncytia formation may proceed as a pathological consequence during covid-19 at low S protein levels and may not be effectively prevented by antibodies."
(2) "Fusion from without" is the process by which particles of some enveloped viruses can direct the fusion of target cells even in the absence of viral replication.
(3) Bratt, M. A., and W. R. Gallaher. 1969. Preliminary analysis of the requirements for fusion from within and fusion from without by Newcastle disease virus. Proc. Natl. Acad. Sci. USA 64:536-543.
(4) Clavel F, Charneau P. Fusion from without directed by human immunodeficiency virus particles. J Virol. 1994 Feb; 68(2):1179-85. doi: 10.1128/JVI.68.2.1179-1185.1994. PMID: 8289347; PMCID: PMC236557.
War against a joker
The pharmaceutical industry and its virologists are currently trying, for transparent reasons, to define the pathogen SARS-CoV2 as a stable hostile entity. For the "war against the virus", the danger is needed, represented by a spiked ball. A "corona-free world" is the declared goal of vaccine-obsessed Bill Gates and his political friends. Also, with regard to a possible vaccination, they try to give us the illusion of a clearly definable enemy in the world of viruses. After all, this is the prerequisite for the testing business and the governmental enforcement of a worldwide vaccination policy that is risk-free for vaccine manufacturers. Today, on 4.5.2020, an online donor conference on the "Creation of a corona-free world" (ARD-Tagesschau) is taking place and Chancellor Merkel promises to spend billions of our tax money on it. From a scientific point of view, all these efforts are - to put it mildly - dangerous aberrations. I am not yet talking about the profiteers of this madness.
Life is not trivial and calculable
It is absolutely certain that the SARS virus is also constantly and rapidly changing. And what good is a vaccination against something that has long since changed incalculably? Our immune system also reacts unpredictably. Cross-immunities? Immune memory? The specificity and significance of tests is quickly fading. So does the effect of a vaccine.
That's why proof of immunity is a farce, and if it becomes law, a health hazard that cannot be justified. For the same reason, mass vaccinations against respiratory viruses are a risky nonsense and may cause bodily injury. With rapidly changing pathogens, as with influenza vaccination, success is a matter of luck. Only afterwards can it be determined whether the vaccinated persons were better off than the non-vaccinated. This remains a good deal, since an evidence-based prior benefit assessment will of course never be possible. Up to now, other viruses have been happy and spread where one type of virus has become difficulties by vaccination.
The Wuhan viruses are long gone
It's all about the extremely high mutation rate of RNA viruses, which includes SARS-CoV2. The rate is impressively demonstrated by the website CoV-Glue, " Amino acid analysis for the SARS-CoV-2 pandemic", which shows that for SARS-CoV2 the mutation rate is very high in a very short period of about 4 months.
· 7237 non-synonymous, i.e. amino acid changing mutations (replacements),
· 6 insertions (inserting additional bases) and
· 87 deletions (loss of bases in the gene sequence) in found gene sequences. .
That is for a genome that itself consists of only about 30,000 bases an enormous number of mutations, insertions and deletions in a very short time. And these are only the data of a few thousand SARS-CoV2 viruses that have been sequenced. Nature knows many, many more. Non-synonymous mutations cause other amino acids to be inserted into the virus' proteins. These thus change the chemical properties of these proteins. These mutations accumulate within weeks(!), as the data show. Insertions and deletions are of special importance, because they can lead to a frame shift, where the whole subsequent chain is read differently. There are also synonymous mutations which, although they do not change the primary structure of the SARS-CoV2 proteins, can still play a role in diagnostics. In addition, there are still many open questions about further effects of synonymous mutations. Doubts about the PCR test, existed from the beginning: Li et al, "Stability Issues of RT-PCR Testing of SARS-CoV-2 for Hospitalized Patients Clinically Diagnosed with COVID-19", J Med Virol. 2020 Mar 26. doi: 10.1002/jmv.25786,
Snapshots of a neverending story
Another important point is that the SARS-CoV2 viruses sequenced so far show an extremely small section of nature. In relation to the total genome of all corona viruses in all humans, this section is of little importance. It must also be remembered that there are not only SARS-CoV2, but also other human coronaviruses - and they also mutate. Otherwise one would not have ended up with the SARS-CoV2 virus. Computer analyses, e.g. of the family tree of SARS-CoV2 (phylogenetic analysis), are very problematic based on this extremely small section of nature as it exists today. For the last 15 years, corona viruses have hardly been considered, neither in humans nor in animals. The vast majority of the coronavirus gene sequences in the databases originate from the last 4 months or are 15 years old. The criticism of this is not new, especially the very inhomogeneous geographical distribution of the gene sequences found, see Mavian et al, "Regaining perspective on SARS-CoV-2 molecular tracing and its implications", medrxiv, 20.3. 2020, : "However, in a new tree inferred just one week later, when more than 135 new full genome sequences were made available on GISAID (Figure S2), the direct link between Germany and Italy has disappeared due to the additional clustering of previously unsampled sequences from Portugal, Brazil, Wales and Netherland (Figure 2b).
Zoonosis? Man is also a zoon!
Some publications say that haplotypes (i.e. genetic patterns) of SARS-CoV2 have already disappeared again, i.e. are no longer found in newly sequenced base sequences. SARS(1) has also disappeared again for a long time. What sense does a genetic distance between two gene sequences make then?
But virology is doing what it has been doing for the last 30 years. It finds a viral gene sequence that it did not yet know and declares the newly discovered virus a death virus. For this to work, it needs the zoonosis hypothesis.
Without it, it doesn't work. Because only thanks to this hypothesis that a pathogen has been newly transferred from an animal host to humans in Wuhan at the fish market at the end of 2019, can a general assumption be made that the pathogen has an increased pathogenicity (= an increased potential to cause illness). The pathogen is new to humans, which is why humans, in contrast to the original hosts, have not had the opportunity to adapt to the new pathogen.
This approach works so well because it is always assumed that patients are seriously ill, who then usually suffer from several diseases (multimorbid), and people with no or weak symptoms are not tested. And immediately you have the apparent proof that positive testing and death go hand in hand.
As proof of this, Drosten, Wieler & Co. hold up two gene sequences, one from an animal corona virus and one from a human corona virus, and point to the large genetic distance. This assertion can be made so easily because there is no data for anything in between. Nobody has measured animal and human coronaviruses in the necessary density in the last 15 years. A very large number of SARS-CoV2 positive people show no or only mild symptoms. The proportion of asymptomatic people who do not show symptoms is said to be 50 - 70%. This is not possible without the immune system having been prepared for the virus. This suggests a continuous development up to SARS-CoV2 (and its many variants).
Talking about origin only shows where you started thinking
Increasingly, phylogenetic analyses are also being carried out in an attempt to construct a different family tree from the numerous different gene sequences; contrary to the hypothesis that SARS-CoV2 was newly created by zoonosis at the end of 2019, this is not the case. Analyses of this kind are problematic due to the very short sample period. However, this is all that is currently available. In addition, the zero point, i.e. the reference sequence against which mutations are evaluated, is arbitrarily chosen. Only in China has the new PCR test been started and the first gene sequences have been generated. Only then did they do the same in other parts of the world. What is a forward and backward mutation is a relative statement in relation to the reference sequence. The supposed spread only reflects the geographical sequence of the tests. Nevertheless, the alarmists at Johns Hopkins continue to use this elsewhere.
We should finally give up the image of a "family tree" - the image of recursive networks appears more appropriate
The diversity of SARS-CoV2 is so great that clusters are formed even in small samples. It is no longer possible to clearly assign how the virus got to New York. Cf. Gonzalez-Reiche et al., "Introductions and early spread of SARS-CoV-2 in the New York City area", April 16, 2020, medxriv: "Phylogenetic analysis of 84 distinct SARS-CoV2 genomes indicates multiple, independent but isolated introductions mainly from Europe and other parts of the United States. Moreover, we find evidence for community transmission of SARS-CoV2 as suggested by clusters of related viruses found in patients living in different neighborhoods of the city." These clusters must have formed in the USA in the last 3 months. It is the SARS-CoV2 and everything that led to SARS-CoV2 is much older.
Alternative interpretations of the same data(!) from the gene databases suggest that SARS-CoV2 has been spreading in humans for 40+ years. See Chaw et al, "The origin and underlying driving forces of the SARS-CoV-2 outbreak", April 14, 2020, bioxriv:
“We have to point out that the TMRCA estimation is strongly influenced by the genome sampling scheme. Since the earliest available genome was sampled on 12/24/2019 almost one month after the outbreak, the real origin of the current outbreak may actually be earlier than our estimation.”
“Assuming a synonymous substitution rate of 2.9x10-3/site/year, the recombination was estimated to have occurred approximately 40 years ago (95% HPD : 31-69 years; divergence time (t) = divergence (dS)/(substitution rate x 2 x 3), considering dS in RBD is 3-fold of genome average). The amino acids in the RBD region of the two genomes have been maintained by natural selection ever since, while synonymous substitutions have been accumulated. If this is true, SARS-CoV-2 may have circulated cryptically among humans for years before being recently noticed.”
These are very recent evaluations and it remains to be seen whether this preprint will make it through the much-vaunted peer review process by which science "regulates" itself and the state of knowledge.
What glyphosate is to fields, antivirals are to humans
Viruses are probably as old as bacteria. The vertebrate immune system is the only one capable of harmonizing the body with the ever-new virus variants. This is exactly what it was created for in the course of evolution. The group of vertebrates originated about 500 million years ago and the concept of the immune system is possibly even older. 500 million years ago, the vertebrate immune system, at the preliminary endpoint of which is man, developed in close contact with the viruses. However, modern medicine uses corticosteroids to suppress the immune response, as shown by many COVID-19 treatment protocols, particularly from the USA.
In the meantime, the industry is constantly advertising new drugs. Where are they used? 98% of test positives show no or only mild symptoms. But the media uncritically mix test and infection, infection and symptomatic disease, symptomatic disease and death. The severely affected persons are 80+ on average and in the vast majority of cases suffer from severe pre-existing conditions. Nobody can say how many of them have died as a result of premature ventilation. In the meantime, intensive care patients are still being weaned off breathing with fentanyl, among other things, otherwise artificial respiration will not work. These patients wake up, if at all, as junkies. Katherine Ellen Foley, "Some drugs used to keep coronavirus patients on ventilators are in short supply", Quartz, March 31, 2020,
The fear is coming out of the ICU, but what's going on?
The ICU's showing what it can do. In addition, there are drugs like Remdesivir, which has been too toxic for the Ebola therapy and fails in further tests. Josh Farkas. "PulmCrit – Eleven reasons the NEJM paper on remdesivir reveals nothing", April 11, 2020, All doubts have not prevented Remdesivir from being released for use in the USA by the flash method. Or chloroquine and azithromycin combination therapies, which can lead to cardiac arrest in people with previous cardiovascular diseases. Or chloroquine monotherapy, which causes damage to red blood cells in people with glucose-6-phosphate dehydrogenase deficiency. Glucose-6-phosphate dehydrogenase deficiency is the most common hereditary genetic defect worldwide, with a frequency of up to 20-30% in Africa. Countries with a high proportion of African-born people are also particularly affected.
Wrong priorities and deceptive figures
Everything is initiated by a dilapidated test, hasty measures and a blind trust in some nano part of the evolutionary machine nature, which is digitized in the gene databases and not
justified by anything. Science and the politicians beleaving its advises will have to continue to pursue their self-made crisis. Although it is very doubtful that a virus that causes no(!)
symptoms in 50 - 70% of infected people had arrived in Europe at the exact time the tests were started, as some now want to make us believe with the help of the curves for excess mortality. And
this in a patient population in which 40% of intensive care patients came directly from the nursing home to the ICU in need of the most intensive care. See Matthias Thöns, "Very wrong priorities set and all ethical principles
violated", Deutschlandfunk, 11.4.2020, "And we have to remember that the seriously ill COVID-19 patients, as the disease is called, are
mostly very old people, many of whom are ill, 40 percent of whom come from nursing homes in need of the highest degree of care, and in Italy, out of 2,003 deaths, only three patients have been
without serious pre-existing conditions. So it is a group that has usually and until now always received more palliative care than intensive care, and now a new disease is diagnosed and all these
patients become intensive care patients." In some countries there is an extra compensation for hospitals, if the DRG is upgraded to
covid-19. This gets still more attractive, if the patient gets intubated. Medicare in US pays 20% more for DRGs with covid-19.
False alarms - a social autoimmune disease
In the current media climate and under immense political pressure to justify the draconian measures and their consequences, even retrospectively, it is very doubtful that there will be an independent scientific discussion on the zoonosis hypothesis of prudent risk assessment. For which research applications will money be granted? Evolution has been going on for millions of years, and in the last 20 years virologists have been conjuring up new death viruses every 3-5 years to threaten humans? MERS, SARS(1), SARS(2), swine flu, bird flu? This has gone really stupid.










Risky vaccination experiments
Dr. Wodarg and Dr. Yeadon apply for immediate stop of all corona-vaccine studies and ask for co-signing their petition
We are asking all European citizens for co-signing the petition. You find the prepared E-Mail to send to the EMA and the text of the petition here.
1.12.2020 Together with the ex-Pfizer head of research Dr. Michael Yeadon, I submitted an application to the EMA, the European Medicine Agency responsible for EU-wide drug approval, on 1 December 2020 for the immediate suspension of all SARS CoV-2 vaccine studies, in particular the BioNtech/Pfizer study on BNT162b (EudraCT number 2020-002641-42).
We call for the studies to be continued - for the protection of the life and health of the volunteers - only once a study design is available that is suitable to address the significant safety concerns raised by an increasing number of renowned scientists against the vaccine and the study design.
As petitioners, we demand on the one hand that, due to the known lack of accuracy of the PCR test, a so-called Sanger sequencing must be used in a serious study. This is the only way to make reliable statements on the effectiveness of a vaccine against Covid-19. On the basis of the many different PCR tests of highly varying quality, neither the risk of disease nor a possible vaccination benefit can be determined with the necessary certainty. For this reason alone, such tests of vaccines on humans are unethical per se.
Furthermore, we demand that it must be ruled out beforehand that risks already known from previous studies, some of which stem from the nature of corona viruses, may have a dangerous effect. Our concerns relate in particular to the following points:
The formation of so-called "non-neutralising antibodies" can lead to an exaggerated immune reaction, especially when test persons are confronted with the real, "wild" virus after vaccination. This so-called antibody-dependent amplification, ADE, has long been known from experiments with corona vaccines in cats, for example. In the course of these trials, all cats that initially tolerated the vaccination well died after being infected with real corona viruses. This overreaction is further encouraged by potentiators.
The vaccinations are expected to produce antibodies against spike proteins of SARS-CoV-2. However, spike proteins also contain syncytin-homologous proteins, which are essential for the formation of the placenta in mammals such as humans. It is essential to rule out the possibility that a vaccine against SARS-CoV-2 could trigger an immune response against syncytin-1, otherwise infertility of indefinite duration could result in vaccinated women.
The mRNA vaccines from BioNTech/Pfizer contain polyethylene glycol (PEG). 70% of people develop antibodies against this substance - which means that many people can develop allergic, potentially fatal reactions to the vaccine.
The much too short duration of the study does not allow a realistic estimate of the late effects. As in the narcolepsy cases after the swine flu vaccination, if emergency approval were planned, late effects would only be observed when it is already too late for millions of vaccinated people. Governments plan to expose millions of healthy people to unacceptable risks and force them to be vaccinated by discriminatory restrictions on unvaccinated people.
Nevertheless, BioNTech/Pfizer apparently submitted an application for emergency approval on 1 December 2020. Scientific responsibility compels us to take this action.
No wonder they sell their own shares quickly!
HERE a sobering scientific commentary in the British Medical Journal (BMJ) on the euphoric announcement of vaccine manufacturers:
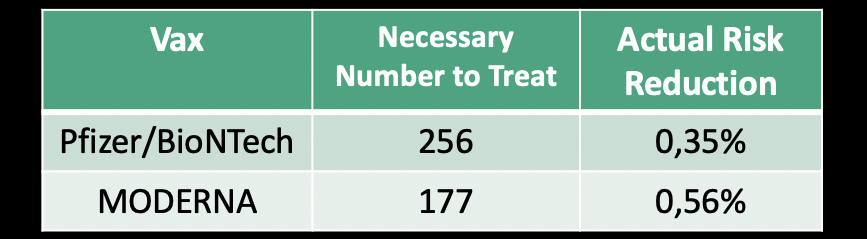
To prevent only one case of Covid-19, 256 people need to be vaccinated with the BioNTech/Pfizer vaccine. With MODERNA it would be 177, so the risky genetic "vaccinations" only help 0.35% and 0.56% of those vaccinated. This is an extremely poor benefit-risk ratio.
Because the other 255 or 176 people have no benefit, but are exposed to the unwanted sideeffects of the vaccines, whatever they may be and whenever we get to know them. A Pfizer top manager probably guessed that others could do better math than many governments and is said to have sold millions of his own shares that very same day.
The test presented today by Moderna with a big press has a similarly low protective effect against Covid-19, an infection that is nothing more than a part of the annual flu.
9.11.2020
Covid-19 – a case for medical detectives
WOLFGANG WODARG, May 2nd 2020,
Before I describe my research on these findings which are very disturbing to me, I would like to say a few words about the assessment of the corona crisis, the reliability of the SARS-CoV-2 PCR test, as well as ubiquitous fear and how it is used politically.
In my investigations into the events after Wuhan, which have completely changed the world since the beginning of 2020, I realized quickly that although we are experiencing a new Corona virus variant, it does not – in view of German data on mortality and morbidity – differ significantly from what has been, or could have been, observed in recent years.
Corona viruses have not been the focus of epidemiological surveillance worldwide, as they have not contributed significantly to globalised seasonal respiratory viral infections, except in the short term in China (SARS 2002/2003) and in the Arab countries (MERS from 2012). There were also no existing vaccines that could have been recombined and marketed annually, as is the case for influenza.
As is well known, regular global episodes of flu have been referred to as "pandemics" since the swine flu of 2009, in an inflationary manner and focusing on single pathogens. In this context, vigilance and historically justified mistrust have long been required. For if our normal, changing and globally circulating viral winter guests, such as the H1N1 viruses in 2009, already meet the criteria of a pandemic, then the term has become meaningless. Before 2009, things were different. At that time, the necessary characteristics of a pandemic included a great many serious illnesses and numerous deaths, with a worldwide catastrophic overload of health care.
To me the sole infection epidemiological aspects of the Wuhan phenomenon are clearly laid out by and large. According to the available figures of the German networks for the surveillance of acute respiratory infections (ARI), the Influenza consortium and the Flu Web, and according to hospital data for ARI, as well as data on the utilization of intensive care units in the country, the flu wave 2019/2020 with its diverse pathogen spectrum has passed without any particularities. Only the consultations in the reporting wards apparently took place much less frequently in the last weeks of the season due to the lockdown.
With regard to acute seasonal respiratory diseases there is currently no reason to fear increased acute respiratory infections. From a medical point of view and considering the available data special precautions are now unnecessary – even if the government says otherwise.
The SARS-CoV-2 PCR test: non-specific, medically useless, but anxiety-producing
Because of the great importance for the Covid-19 occurrence, special attention must be paid to the SARS-CoV-2 PCR test – the only instrument available to measure the virus and to be able to talk about a new spread at all. My assessment on this has not changed since the end of February: Without the PCR test for SARS-CoV-2 viruses designed by German scientists, we would not have noticed a corona "epidemic" or even a "pandemic".
After the WHO recommended it ("not for medical diagnostic purposes"), the test was used all over the country in the attempt to find fragments of SARS virus. An institution in China, whose name was not mentioned by one of the developers of the PCR test, Prof. Drosten, during an interview on German public radio “Deutschlandfunk”, confirmed to the virologist that the test used by him found the SARS fragment they were looking for in the Wuhan SARS virus.
My assessment of this test which is not officially accredited and not approved for medical purposes and now used to search for "cases" worldwide, is as follows:
How can a test that turns out positive for the many different SARS viruses of bats, dogs, tigers, lions, domestic cats and humans, which have been changing and spreading worldwide for many years, be called specific for the detection of an allegedly only four-month-old SARS-CoV-2?
Apparently it is a sensitive test that produces too many positive results. Therefore it can also detect many – in the meantime naturally recombined – SARS-like pathogens. This does not deny that the viruses from Wuhan were also among those.
However, the test seemingly also measures earlier SARS variants that are constantly altering, can change hosts quickly and are not found in virologists' databases. However, these were and are obviously not considered to be extraordinarily dangerous.
So how do we know that the discrepancy between the many harmless infections and the few more severe courses is not due to the fact that different variants are found equally well with the test used? Especially since it turns out positive even for animal variants!
However, a positive – although possibly meaningless – test result is always frightening and causes an immediate and predictable respective behaviour on the part of those affected and those responsible. The widespread testing, the fixation on ventilation problems, the emptying of the clinics for the announced flood of Covid-19 victims and triage exercises caused panic and thus guaranteed the obedience of a strongly intimidated population.
How to make fear last
When it became increasingly clear – even before the lockdown measures – that Germany would probably be mostly spared, two new foreign images of horror dominated the reporting in our country and ensured that fear and obedience continued: coffins and deadly chaos in many Italian and Spanish hospitals, refrigerated containers full of corpses and mass graves in New York. The conclusion was, that it had to be a dangerous epidemic after all.
However, it is unlikely that the same virus is so much more harmless in Hamburg than in New York. There must be other reasons for this.
Therefore I focused my research on these new focal points of the recent development. Perhaps, I hoped, it would then be easier to understand why many governments keep talking about the threat of
a "second wave" and the continued need for a lockdown.
It is currently reasoned that the measures should be maintained more or less until the entire population can be saved by vaccination. One and a half years of a "new normality" without holidays,
celebrations, cultural and sporting events are demanded and compulsory vaccinations, compulsory tests, tracking and immunity apps are held in prospect.
But why? How can the government be so sure to consider it necessary to repeal essential parts of the Basic Law, to drive the middle class into bankruptcy and to let workers and employees fall into unemployment? What else are we facing?
Medical Detectives: A look beneath the surface
The challenge is to find out what happened, for example, in Northern Italy, Spain or New York. In order to grasp this more research is needed, than what is taught in normal epidemiology. In Baltimore, at the now unfortunately institutionally corrupted Johns Hopkins University, I used to attend intensive epidemiological training, which gave me a great deal of methodological knowledge. There was also a branch called "Medical Detectives".
Here one could learn from history and on the basis of numerous well-researched cases how health consequences can arise, for example, from well or food poisoning and which tricks make it difficult to distinguish natural from man-made or even criminal causes. Medical detectives – everyone knows it from crime novels – have perpetrators and victims, motives and murder weapons, alibis and clients.
A disease – even one declared by the WHO – can be a "fake". In the cases of bird flu and swine flu, I have seen and investigated the unscrupulous and corrupt machinations of a pharmaceutical and vaccine industry. Time and again health fears have been created to divert billions of public money into private pockets with dangerous products.
That is why one may also ask about Covid-19: Could there be something else behind the public's continued anxiety? Qui bono? Who benefits from the fear?
Virologists once again as fear-mongers
Besides the WHO, the fear-mongers are again some virologists I already know from the past. Most of them – and this is unfortunately already "new normality" everywhere at medical institutes today – have established close cooperation with the pharmaceutical industry or other investors.
Nowadays it is easier to become a professor if you have shown skills in obtaining third-party funds. Science has become accustomed to "cheating", and the universities make this easier through non-transparent spin-offs, public-private partnerships or cooperation with alleged charitable foundations.
The virology department of the Berlin Charité is supported by the Bill and Melinda Gates Foundation regarding Covid-19. A co-author of the PCR test by Drosten et al. is the CEO of the biotech company TIB Molbiol, which is now increasingly producing tests and selling them for millions. However, these are detective secondary findings that do not explain by far what is turning this world upside down.
The majority of experts can no longer deny that the danger of infections in Germany and its neighbouring countries has already passed, without embarrassing themselves for the rest of their careers. And yet there are people in governments, public offices and the scientific community who want to lock us up with fear and keep on patronizing us.
My annoyance about this medically incomprehensible panicmongering and about many epidemic-hygienically nonsensical authorizations and freedom-withdrawing disciplinary measures is also accompanied by the curiosity of a "medical detective" who is concerned about possible hidden motives. Nevertheless, I do not want to deal with the political or economic background at this point. The time for this will probably come eventually. Moreover it is not my area of expertise.
Are we facing a "second wave"?
The question I ask myself is: How was it possible to create such horror scenarios with an apparently relatively harmless pathogen, whereby critics could be effortlessly eliminated and the fear in the population could constantly be fed by the media?
I would also like to know based on what scientific evidence the German Chancellor, her Minister of Health, her “virologist of choice” and others continue to announce: The second wave is yet to come. It will take many more months. We must not go on holiday. We have to be prepared to work from home in the future. We all have to be tested, tracked and vaccinated with a drug that has yet to be tested. Although all this is already laid out in the script with the title "The first modern pandemic", published by Bill Gates on April 23, it is not medically explained there either.
A hint from New York
On March 31 I received an important tip: New York intensive care physician Dr. Cameron Kyle-Sidell had alerted his colleagues with an astonishing observation. He reported:
"The Patients I saw in my ICU, they were no Covid-19 patients. They didn't have any signs of pneumonia, but rather looked like passengers on a plane, that suddenly lost pressure at high altitude."
Therefore It had to be a disturbance of the oxygen transport in the blood. I researched and ticked off the various known causes of such symptoms one after the other, if they were out of the question because of the progression of the disease. The most probable cause seemed to be rapid hemolysis, a destruction of the erythrocytes (red blood cells) that exchange oxygen in the lungs for Co2 to exhale in order to transport the oxygen to every corner of our body. Patients then feel suffocated, breathe very quickly and under great effort.
We know what to do in such a case because it is demonstrated to us in the aircraft before every take-off: Oxygen masks fall from the ceiling and bring relief until everything is back to normal. This is exactly what helped the patients in New York the best. Intubation and ventilation, on the other hand, were wrong and killed people in many places.
The Nigerian dead in Sweden
I was aware of such a case with the same puzzling symptoms, which had been described in 2014 by
Swedish pneumologists in a young patient from Nigeria who had died of the disease. At that time, an enzyme deficiency was suspected and actually found to be a possible cause after death, which
occurs in many regions of Africa in 20 - 30% of the population.
It is the so-called glucose-6-dehydrogenase deficiency, or "G6PD deficiency", one of the most common genetic peculiarities, which can lead to threatening haemolysis (dissolution of red blood
cells), mainly in men, when certain drugs or chemicals are taken. The following map shows the distribution of this deficiency (Source and explanations here).

This hereditary trait is particularly common among ethnic groups living in areas with malaria. The modified G6PD gene offers advantages in the tropics. It makes its carriers resistant to malaria pathogens. However, G6PD deficiency is also dangerous if those affected come into contact with certain substances found in, for example, field beans, currants, peas and a number of medicines.
These include acetylsalicylic acid, metamizole, sulfonamides, vitamin K, naphthalene, aniline, malaria drugs and nitrofurans. The G6PD deficiency then leads to a disruption of the biochemical processes in the red blood cells and – depending on the dose – to mild to life-threatening haemolysis. The debris of the burst erythrocytes subsequently leads to microemboli, which block small vessels throughout the organs. What had caused the illness and death of the young man from Nigeria remained unclear at the time.
An alarming discovery
I looked at the drugs that can cause severe hemolysis in G6PD deficiency and got really scared. One of the substances that is called very dangerous in all forms of this enzyme deficiency is the anti-malarial drug hydroxychloroquine (HCQ).
But this is precisely the substance that Chinese researchers in Wuhan have been recommending against SARS since 2003. Along with the virus from Wuhan, HCQ now came back to us as one of the therapeutic options and was accepted as such. At the same time, HCQ was recommended as a promising agent against Covid-19 for further clinical trials with the support of WHO and other agencies.
According to reports, production of this drug is to be increased in Cameroon, Nigeria and other African countries. India is the largest producer of HCQ and exports it to 55 countries. Werner Baumann, Chairman of the Board of Management of Bayer AG, announced at the beginning of April that "various investigations in laboratories and clinics" had provided first indications that chloroquine might be suitable for the treatment of corona patients. The company then provided several million tablets.
There are now hundreds of trials worldwide, planned or ongoing by different sponsors, in which HCQ is used alone or together with other drugs. When I looked at some large studies to see if patients with G6PD deficiency were excluded, I found no evidence of this in most study plans. In the USA, for example, a large multi-center study with 4,000 volunteers from healthy medical staff is being prepared. Here, however, the term "hypersensitivity" is only used in general terms, as is the case with all drugs with regard to allergic reactions. In a chloroquine/hydroxychloroquine study by Oxford University (NCT04303507) with a planned 40,000 participants, the risk of G6PD deficiency is also not mentioned. In another large study by the Pentagon, though, there is an explicit warning to exclude G6PD deficiency patients from the study.
The following graph, based on information from the WHO database, shows how many studies on Covid-19 and HCQ have been initiated – and how few of them take enzyme deficiency into account.

Mostly only the cardiac complications of chloroquine or hydroxychloroquine are mentioned, which in Brazil led to the premature termination of a study with 11 deaths of 81 subjects. However, it seems that worldwide little attention is paid to this further serious side effect. In addition, due to the lack of alternatives, HCQ has been tolerated and massively applied in many countries since the beginning of the year as part of a so-called "compassionate use". In medicine, compassionate use refers to the use of not yet approved drugs in emergency situations.
Conspicuous clusters
During this research, more and more results of more precise evaluations of the deaths in especially affected cities were received. In New York and other cities in the USA, it was reported that the vast majority of fatalities were African Americans – twice as many as could be expected based on the proportion of the population.
Also from England, where the mortality data from Euromomo shows an increasing death rate since the beginning of April, it was reported that 35% of about 2000 seriously ill people, twice as many as expected, came from ethnic "minorities" ("black, Asian or other ethnic minority"), including doctors and medical staff.
A major doctor's death in Italy remains in urgent need of clarification. The death of about 150 doctors and only a few female doctors is associated with Covid-19. Although age may have played a role in many of these cases, it should be noted that a high prevalence of G6PD deficiency has also been described for some regions of Italy and that in Italy up to 71% of those who tested positive with PCR, as well as the staff, had a prophylactic high level of HCQ. The same applies to Spain. Among the first 15 Covid-19 deaths in Sweden, there were 6 younger migrants from Somalia.
Deadly combination
Therefore the frightening result of my research is that typical severe courses with haemolysis, microthrombi and shortness of breath without typical signs of pneumonia occur more frequently where two factors come together:
- Many patients with ancestors from malaria countries with G6PD deficiency
- Prophylactic or therapeutic use of high-dose HCQ
This is exactly what is to be expected in Africa, and this is already the case everywhere where migration is causing a large proportion of the population coming from malaria countries. The following diagram shows the process flow schematically.

Cities such as New York, Chicago, New Orleans, London, or even large cities in Holland, Belgium, Spain and France are such centers. If the test is widely used in these migration hotspots and is expected to be positive in about 10 to 20% of the population, many people from the G6PD countries will also be among them. If they are then treated with high-dose HCQ, either prophylactically or as part of a "compassionate" use, as planned, then those severe clinical pictures will also be evoked in young people, as has been presented to us by the sensational press, and which keep our fear of Covid-19 alive.
It is unknown how many times this deadly combination has already led to victims. There has been no discussion of the issue among those responsible in the WHO and in governments. There is also a frightening lack of knowledge and sense of responsibility among doctors who are accountable for the treatment of Covid-19 patients or for the staff treating them.
Once again: This connection applies not only to Africa, but also to large parts of Asia, South and Central America, Arabia and the Mediterranean region.
However, the cases mentioned have nothing to do with Covid-19 disease. A PCR test result leading to the prophylactic prescription of HCQ is sufficient to cause severe disease in up to one third of the people from high-risk populations treated in this way.
HCQ treatment for G6PD deficiency is a dangerous malpractice
This could be remedied immediately if all treating physicians worldwide were informed about the contraindication of HCQ. However, the WHO, the CDC, the ECDC, the Chinese SARS specialists, the medical associations, the drug authorities and the German government and its advisors are carelessly neglecting to inform the public. In view of the ongoing programmes, this appears to be gross negligence.
It is a malpractice to treat people with G6PD deficiency with high-dose chloroquine derivatives or other drugs known to be dangerous for them. Under the WHO label "'Solidarity' clinical trial for COVID-19 treatments", healthy people are exposed in a hurry to authorised, life-threatening experiments. Hundreds of clinical trials, mostly worthless observational studies with parallel approaches, very often also run with HCQ as one of the alternatives.
German drug legislation prohibits the use of unauthorised drugs, but the government still encourages this. A non-validated test that is not approved for diagnostic purposes provides the pretext for the use of life-threatening medication – given an infectious disease where there is still no evidence that it poses serious risks beyond the risk of the annual flu epidemic.
At full throttle into the catastrophe
The dangers of this epidemic are presented with the help of scientific imposture. An unsuitable test from Berlin provides the pretext for deadly measures all over the world. The consequences of these mistakes lead to emergencies in many regions, which are attributed to an epidemic. This creates precisely the wave of fear so many in business and politics are now riding and which threatens to bury our fundamental rights.
The public, the media and the medical community hardly seem to be surprised that in New York and other centres more than twice as many "African Americans" die as would be expected due to their population share. Even in the studies of deaths in the USA and elsewhere, the risk posed by G6PD deficiency is almost always ignored or forgotten.
When sought-after virologists and other experts have been announcing for a long time that there will be a wave of deaths and terrible conditions in the cities in Africa, do they know about these connections? Or are there other provable reasons that justify such momentous prophecies? Finally: Is all this just a matter for science or also for public prosecutors and courts?
Note from the editor: Further information and graphics can be found on the author's website.
About the author: Dr. med. Wolfgang Wodarg, born in 1947, is an internist and pulmonary physician, specialist for hygiene and environmental medicine as well as for public health and social medicine. After his clinical activity as an internist, he was, among other things, a public health officer in Schleswig-Holstein, Germany for 13 years, at the same time lecturer at universities and technical colleges and chairman of the expert committee for health-related environmental protection at the Schleswig-Holstein Medical Association; in 1991 he received a scholarship at the Johns Hopkins University, Baltimore, USA (epidemiology).
As a member of the German Federal Parliament from 1994 to 2009, he was initiator and speaker in the Enquête Commission "Ethics and Law of Modern Medicine", member of the Parliamentary Assembly of the Council of Europe, where he was chairman of the Subcommittee on Health and deputy chairman of the Committee on Culture, Education and Science. In 2009, he initiated the Committee of Inquiry into WHO's role in H1N1 (swine flu) in Strasbourg, where he remained as a scientific expert after leaving Parliament. Since 2011 he has been working as a freelance university lecturer, doctor and health scientist and was a volunteer member of the board and head of the health working group at Transparency International Germany until 2020.
1.3.2020 Corona-Hype:
Without PCR-Tests there would be no reason for special alarms.
We are currently not measuring the incidence of coronavirus diseases, but the activity of the specialists searching for them.
by Wolfgang Wodarg
The corona hype is not based on any extraordinary public health danger. However, it causes considerable damage to our freedom and personal rights through frivolous and unjustified quarantine measures and restrictions. The images in the media are frightening and the traffic in China's cities seems to be regulated by the clinical thermometer.
Evidence based epidemiological assessment is drowning in the mainstream of fear mongers in labs, media and ministries.
The carnival in Venice was cancelled after an elderly dying hospital patient was tested positive. When a handful of people in Northern Italy also were tested positive, Austria immediately closed
the Brenner Pass temporarily.
Due to a suspected case of coronavirus, more than 1000 people were not allowed to leave their hotel in Tenerife. On the cruise ship Diamond Princess 3700 passengers could not disembark., Congresses and touristic events are cancelled, economies suffer and schools in Italy have an extra holyday.
At the beginning of February, 126 people from Wuhan were brought to Germany by plane and remained there in quarantine two weeks in perfect health. Corona viruses were detected in two of the healthy
individuals.
We have experienced similar alarmist actions by virologists in the last two decades. WHO's "swine flu pandemic" was in fact one of the mildest flu waves in history and it is not only migratory
birds that are still waiting for "birds flu". Many institutions that are now again alerting us to the need for caution have let us down and failed us on several occasions. Far too often, they are
institutionally corrupted by secondary interests from business and/or politics.
If we do not want to chase frivolous panic messages, but rather to responsibly assess the risk of a spreading infection, we must use solid epidemiological methodology. This includes looking at
the "normal", the baseline, before you can speak of anything exceptional.
Until now, hardly anyone has paid attention to corona viruses. For example, in the annual reports of the Robert-Koch-Institute (RKI) they are only marginally mentioned because there was SARS in China in 2002 and because since 2012 some transmissions from dromedaries to humans have been observed in Arabia
(MERS). There is nothing about a regularly recurring presence of corona viruses in dogs, cats, pigs, mice, bats and in humans, even in Germany.
However, children's hospitals are usually well aware, that a considerable proportion of the often severe viral pneumonia is also regularly caused or accompanied by corona viruses worldwide.
In view of the well-known fact that in every "flu wave" 7-15% of acute respiratory illnesses (ARI) are coming along with coronaviruses, the case numbers that are now continuously added up are still completely within the normal range.
About one per thousand infected are expected to die during flu seasons. By selective application of PCR-tests - for example, only in clinics and medical outpatient clinics - this rate can easily
be pushed up to frightening levels, because those, who need help there are usually worse off than those, who are recovering at home. The role of such s selection bias seems to be neglected in
China and elsewhere.
Since the turn of the year, the focus of the public, of science and of health authorities has suddenly narrowed to some kind of blindness. Some doctors in Wuhan (12 million inhabitants) succeeded
in attracting worldwide attention with initially less than 50 cases and some
deaths in their clinic, in which they had identified corona viruses as the pathogen.
The colourful maps that are now being shown to us on paper or screens are impressive, but they usually have
less to do with disease than with the activity of skilled virologists and crowds of sensationalist reporters.
We are currently not measuring the incidence of coronavirus diseases, but the activity of the specialists searching for them.
Wherever such the new tests are carried out - there are about 9000 tests per week available in 38 laboratories throughout Europe on 13 February 2020 – there are at least single
cases detected and every case becomes a self-sustaining media event. The fact alone, that the discovery of a coronavirus infection is accompanied by a particularly intensive search in its
vicinity explains many regional clusters.
The horror reports from Wuhan were something, that virologists all over the world are waiting for. Immediately, the virus strains present in the refrigerators and computers were scanned and
compared feverishly with the reported newcomers from Wuhan. A laboratory at the Charitè in Berlin was the first to be allowed to market its in-house tests worldwide. Not as a licenced medical product, but as a recommended test by
WHO, and not to be used for diagnostic purpose. Prof C. Drosten was interviewed on 23rd of january 2020 and described how the test
was established.
He said, that he had heard about a new virus in China from social media on the last days in 2019 and immediately has rememberd his experience with chinese SARS - species from 2003 and after. So
he took all those SARS -sequences he reached and constructed some primers. His friend and partner for many years, who had a specialized Lab in Berlin and helbed him do realize a test set,that
they sent to Wuhan.. Tey were cooperating with a Partner from China, who confirmed the specific sensitivity of the Charitè-Test for the Wuhan coronavirus. The virus itself was only identified as
a digitalized sequence and has never been isolated or proven to be the SARS-CoV-2 pathogene agent in search. Other tests from different places followed soon and rapidely found their
market.
However, it is better not to be tested for corona viruses. Even with a slight "flu-like" infection the risk of coronavirus detection would be 7% - 15% . This is, what a prospective monitoring in Scotland (from 2005 to
2013) may teach us. The scope, the possible hits and the significance of the new tests are not jet validated. It would be intersting to have soe tests not only on airports and cruising ships
but on german or italian cats, mice or even bats.
If you find some new virus RNA in a Thai cave ore a Wuhan hospital, it takes a long time to map its prevalence in different hosts worldwide.
But if you want to give evidence to a spreading pandemic by using PCR-Tests only, this is what should have been done after a prospective cross sectional protocoll.
So beware of side effects. Nowadays positive PCR tests have tremendous consequences for the everyday life of the patient and his wider environment, as can be seen in all media without
effort.
However, the finding itself has no clinical significance. It is just another name for acute respiratory illnesses (ARI), which as every year put 30% to 70% of all people in our countries more or
less out of action for a week or two every winter.
According to a prospective ARI-virus
monitoring in Scotland from 2005 to 2013, the most common pathogens of acute respiratory diseases were: 1. rhinoviruses, 2. influenza A viruses, 3. influenza B viruses, 4. RS viruses and 5.
coronaviruses.
This order changed slightly from year to year. Even with viruses competing for our mucous membrane cells, there is apparently a changing quorum, as we know it from our intestines in the case of microorganisms and from the Bundestag in the
case of political groups.
So if there is now to be an increasing number of "proven" coronavirus infections. in China or in Italy: Can anyone say how often such examinations were carried out in previous winters, by whom,
for what reason and with which results? When someone claims that something is increasing, he must surely refer to something, that has been observed before.
It can be stunning, when an experienced disease control officer looks at the current turmoil, the panic and the suffering it causes. I'm sure many of those responsible public health officers
would probably risk their jobs today, as they did with the "swine flu" back then, if they would follow their experience and oppose the mainstream.
Every winter we have a virus epidemic with thousands of deaths and with millions of infected people even in Germany. And coronaviruses always have their share.
So if the Federal Government wants to do something good, it could learn from epidemiologists in Glasgow and have all clever minds at the RKI observe prospectively (!!!) and watch how the virom of
the German population changes from year to year.
Some questions for the evaluation of the current findings:
- Which prospective, standardised monitoring of acute respiratory diseases with or without fever (ILI, ARI) is used for the epidemiological risk assessment of coronavirus infections observed in Wuhan Italy, South Korea, Iran and elsewhere (baseline).
- How do the comparable (!) results of earlier observations differ from those now reported by the WHO? (in China, in Europe, in Italy, in Germany, etc.)
- What would we observe this ARI-season if we would ignore the new PCR-testing?
- How valid and how comparable are the detection methods used with regard to sensitivity, specificity and pathogenetic or prognostic relevance?
- What is the evidence or probability that the observed corona viruses 2019/2020 are more dangerous to public health than previous variants?
- If you find them now, how can you proove, they were not there (e.g. in animals) before.
- How do you make shure, that a positive tested case is not in the same time suffering/dying from other virus co-infections?
- What considerations have been made or taken into account to exclude or minimise sources of bias (sources of error)?